“A real house,” says Edwin. “A dog. A girlfriend. And making a little music.”
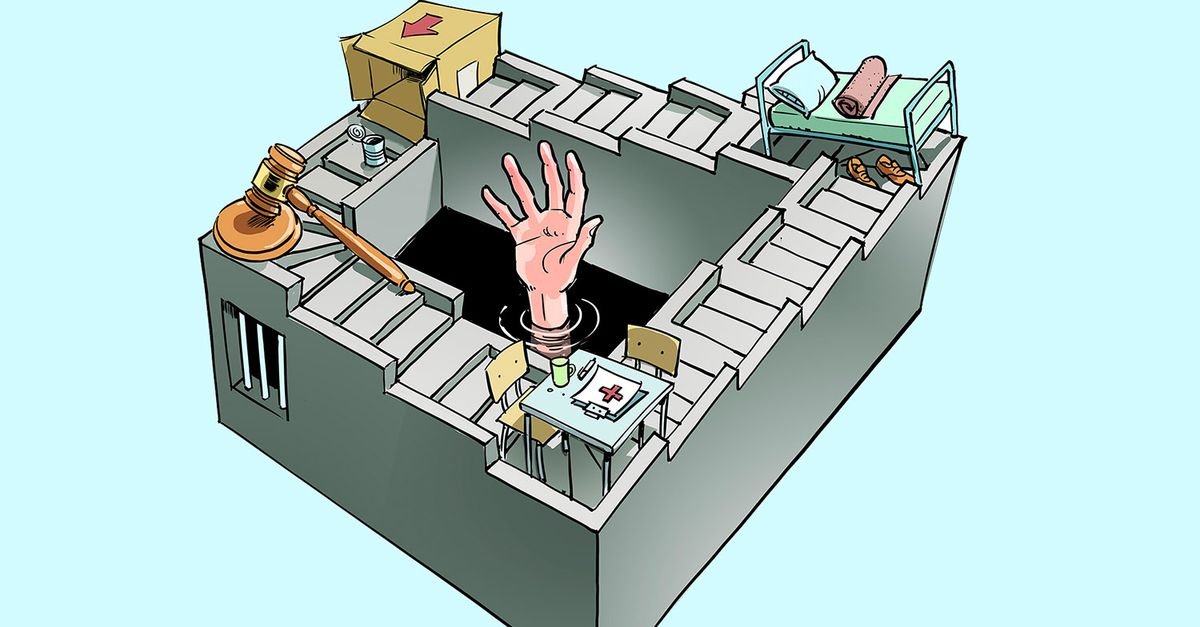
If he can and dares to dream, that is his wish. Spoken in a moment of clarity, somewhere between two psychoses, somewhere between two police stations. Edwin lived in the space between systems for more than twenty years. Too complex for mental health care, too unstable for homeless shelters, too requiring care for prison. So he commutes. Crisis shelter, street, courtroom, police station. Over and over again. Sometimes with a period of stability and hope, in which he dreams of a dog.
Journalist Bas Haan (NRC) writes in his book Deadly care about Edwin, who eventually becomes so desperate due to inadequate care and failing systems that he hangs himself in a police cell. Josephine Lenssen, medical director of the mental health institution that had to care for Edwin, recently responded NRC (5/6): “I cannot keep those people in my clinic if it is not efficient.”
On June 9, Jason Bhugwandass presented his report Died lonelythe successor to his earlier report Lonely closed from 2024, about the abuses in the two ‘very intensive short-term observation and stabilization’ departments (ZIKOS) in closed youth care. Bhugwandass stood in a suit, behind a coffin. Surrounding it are photos of seven young people who died after a ZIKOS placement. He read out the names of the fifty-one young people he spoke to for this report. Thirty-eight of them attempted suicide between the two reports.
Bhugwandass’s first report caused a commotion and parliamentary questions. Both ZIKOS departments closed, the only one of the seven recommendations from his report that was followed. Only now, after his second report, did an apology come from the responsible institutions. What also came was a flood of responses from all kinds of passionate care providers and administrators. The semi-reliant Netherlands hastened to contribute.
They undoubtedly mean well. Everyone who writes something means it. Friso van Doesburg, expert and trainer in youth care, wrote a nice response on LinkedIn in which he calls on youth care professionals to look at things differently. His recently published book Basic posture is a plea for humanity: relationship as a foundation, neurobiology as substantiation, presence as intervention. So as a care provider you don’t want to change the young person, but rather be there and seek connection – even if he pushes you away, even after the umpteenth time. He’s right.
The beds are not there
I know the young people Bhugwandass writes about. Young people who are locked up for their ‘safety’ and are therefore further damaged. I know the Edwins in the making, young adults who are passed on like a hot potato from one “chain partner” to another. And I know Friso is right. The basic attitude makes the difference. I see it every day.
That makes it all the more painful that he and the vast majority of healthcare professionals I speak to leave the most important part of the solution unmentioned.
There is no good help for the Edwins and the young people who died alone. But that is not because care providers do not want to connect, or because they do not know neurobiology. It’s because the beds aren’t there. Not the time per client. Not the continuity. The familiar face that comes back, even if you’ve sent it away six times, doesn’t. All that costs money. And that money is there, but it is somewhere else. Where it is, and why that is the case, are questions that many care providers do not dare to ask.
Take Edwin. Despite a long-term care authorization, admission was not effective. But what exactly does that term mean? When is something efficient? Whose ‘goal’ is it really about, and why is that even a factor in sheltering desperate people?
‘Efficiency’ is primarily a financial incentive. It sounds like a substantive question: is this the right place, the right help, for this person? And that is how medical director Lenssen means it. But in a system that runs on billable hours, that demand shifts unnoticed. ‘Is this the right help?’ becomes ‘can we justify this aid?’ And ‘can we justify it?’ ultimately becomes: ‘will we get paid?’ Edwin’s goal — a house, a dog, a little peace and quiet — didn’t fit into any of those questions.
No matter how often we proclaim the right basic attitude, humanity cannot be institutionalized in a system that runs on cost price logic.
Machine of carefulness
Emergency workers are generally very good people. I say that without irony. They continue to work with perseverance in a field where the problems and backlogs are increasing. They often do more than they are paid for. They also know that things have to be different and can quickly recite the main ingredients for better care.
But as soon as it comes to the distribution of wealth – about the question of why there is money for some people and not for others – they become silent. Lenssen also just doesn’t get there. When I question that system and the growing inequality in the Netherlands, they respond as if I were complaining about the weather. Wasted effort: the system as an elusive and unchangeable truth that we can only accept.
Care providers prefer to carefully divide a pie that is much too small. And that care has a price; indications, tenders, supervisors, accountability systems, quality registrations. We spend so much energy determining whether the money we spend is sufficiently responsible that there is even less money left for actual care. We built a machine to prevent waste, but that machine is the waste.
Bas Haan and Michelle van Tongerloo’s book A country comes to the doctor provides a sharp analysis of how political and economic fantasies have destroyed healthcare. Decades of cutbacks presented as efficiency measures, market forces as a healthcare philosophy, an army of administrators and advisors, and aid that is only financed when the problems are large enough to declare.
If the fire brigade were organized in the same way, as a firefighter I would first have to ask for water, stating where, when and what type of fire will occur. I would then be given a plant sprayer because it was estimated that this would be able to extinguish the fire. If it appears that the fire is getting bigger, I am allowed to switch to a powder extinguisher, and only when the entire house is ablaze am I given permission to set up the fire hose.
Why is this scenario in a fire so obviously absurd and why do we accept it among people?
We built a machine to prevent waste, but that machine is the waste
The solution does not start in healthcare. It starts with the question: why is the cake so small? So in addition to basic attitudes and humanity, it must also be about taxes. A discussion about fixing healthcare is pointless without also talking about the distribution of wealth. About what happens to a society when that distribution becomes increasingly skewed. About what we are willing to collect from people who have a lot, in order to invest in people who have little. Provide assistance is politics. If, as an aid worker, you are not concerned with distributing prosperity, you are sweeping the floor with an open tap.
The next Edwin is coming. The next Kira, Julia, Tara, Tamara, Simone and Indra are in the making. There is the will to prevent that. The money needed to really do things differently is simply there. The Netherlands is one of the richest countries in the world. We choose together where that wealth ends up.