Powerful influence, hidden networks in state care, expropriation of assets, professional monopoly – just a few phenomena that can be associated with the medical barons. The power of today’s medical barons is not in the envelope, but in the structures, and not only the patient but also the system depends on it, it can be read Possibilities for the downsizing of medical bar structures in Hungarian healthcare in the discussion paper, which the Hungarian Medical Chamber (MOK) a on his website published.
According to the MOK’s experience, the removal of gratuity was a step of historical importance, but the baronial structures continue to live on today, just in a different way: in positions, appropriated knowledge and relationships.
The power of medical barons goes beyond their professional position
But who do we call medical barons in common parlance? In 2016, this term appeared for the first time in a newspaper article. This name applies to those in a position of power, who have large financial resources and the ability to influence the health sector. The system of doctor oligarchs was formed during socialism and then strengthened with economic and political connections.
It is important to mention, and the IOC also highlighted, that the medical baron is not the same as the medical professional elite, although there may be personal overlaps between them. Every country’s medical society has its professional elite. They are the ones “who, through their personal ambition, abilities and diligence – thus their merits – occupy a leading role in the medical community”. In contrast, the medical barons are defined by their power operation. Medical barons make up roughly 1-3 percent of the medical community.
The MOK’s starting point is that the medical oligarchs can significantly influence Hungarian healthcare. Due to their influence, decisions are often made not according to professional, but personal, economic or political interests. This hinders the renewal, efficiency and safety of healthcare.
So, indirectly, the medical barons are obstacles to a more modern and fair health care.
The embeddedness of the medical barons is shown by the fact that, in many cases, certain surgical techniques are only available to them, and they decide who is allowed to “learn by the operating table”.
These doctors often have their own equipment, and a relationship is also established between the barons and the industrial players. The companies depend on where the medical manager orders the therapeutic or diagnostic devices from, so most of the orders are made through overpriced public procurement procedures, writes the MOK.
After the elimination of the gratuity, the private sector became the tool of the medical barons
Although you might think that the power of the medical barons ended with the end of the gratuity in 2020, in fact it didn’t happen that way. The reason for this is that in 2021 the wage increase, which is still considered significant, did not cover the loss of the gratuity for a baron doctor. Therefore, many people looked for a way out so that their financial and social status would not be lost. The IOC writes: initially, many people simply continued their illegal activities, but when the first came to light detentionsthey tried to come up with creative solutions.
Those involved quickly adapted: they continued to build their influence in the private healthcare sector. The medical barons were able to expand by “crossing over” between the public and private sectors, which was forbidden in principle. In other words, in practice, the same patient was treated in both public and private care. Then came the fact that “the inspection fee of hundreds of thousands had to be paid privately, or cars with rolled-down windows in the parking lot served as mailboxes for the envelopes,” writes the MOK.
The increase in demand for the private sector was “good for the medical barons”. This culminated when the capacities of the public health sector were reduced due to the coronavirus epidemic, and the population could only access more care in the private sector. We also wrote about the fact that every third forint spent on health care goes to private providers, and not to the classical health-financed gets to institutions. “Private clinics were opened one after the other, investments worth billions took place, in a few years there was a 40 percent increase in the sector, and a business of HUF 1,000 billion was created annually,” writes the MOK.
The private sector became the tool of the medical barons, despite the fact that the law wanted to separate the two sectors from each other.
In this situation, the increase in state waiting lists was even beneficial for the medical barons: it had a direct business-boosting force. Then, with a little delay, a new form also emerged: some state hospitals started to create private channels through foundations and internal companies that were officially separated, but in reality based on state care. A good example of this was one of the chronic departments of the Péterfy Hospital, where, as it turned out: they could ask patients for HUF 160,000 per month.
The careers of almost half of the doctors were negatively affected by the presence of the medical barons
Péter Takács, the current Secretary of State for Health, in an interview in 2024 promised to that he will exterminate the medical barons with “fire and iron” because of which the waiting lists for surgery are longer. This did not turn out to be so successful in the end. At the beginning of December 2025, the chamber conducted a survey based on a sample of 4,000 people on the conditions of private and public health care, and on the phenomenon of medical barons. This was published on April 21.
In the survey, respondents were asked whether medical barons exist, to which 93 percent of respondents answered yes. The careers of almost half of the doctors were negatively affected by the presence of the medical barons:
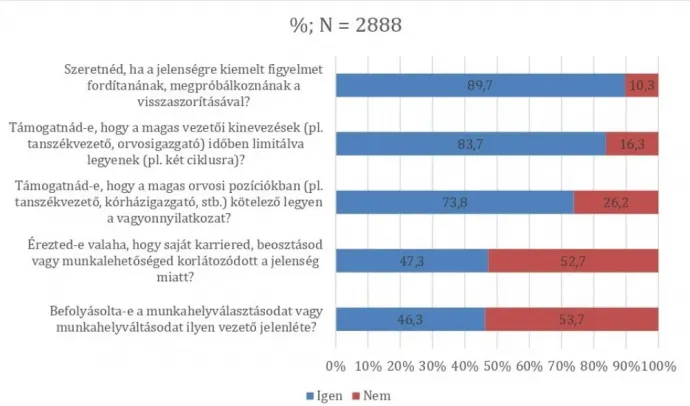
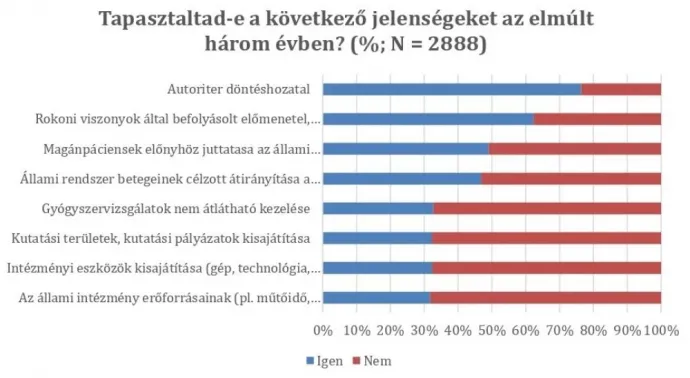
More than 70 percent of respondents experienced authoritarian leadership in the last three years:
The vast majority would support time limits on managerial appointments and public asset declarations.
MOK: Transparent appointments and promotions are needed
In March 2024, Péter Magyar spoke about the radical transformation of the health sector, the replacement of the medical barons you can’t wait a minute. According to Magyar, every minute of delay can cost human lives. The IOC also formulated proposals that, according to them, could really reduce the power of the medical barons in the future.
The listed suggestions are not exhaustive:
- Management positions (head of department, head of department, center president) should be tied to a time-limited mandate (for example, 2×4 years).
- The condition for reapplying should be the result of an independent professional and ethical evaluation.
- There should be transparent appointment and promotion criteria.
- All management candidates must fill out a declaration of conflict of interest (indicating family, economic and professional relationships).
- Young specialists (and civilians) are involved in professional colleges and policy-making.
- All accredited training, surgical procedures and protocols should be accessible on a national platform.
- Institutional performance indicators should be made public (for example, surgical case numbers, waiting lists, medical performance indicators, patient complaints).
- Managerial benefits should be made public.
- In the case of senior managers, the asset declaration should be made public (this is also the practice in Romania, for example).
- Make research and tool use decisions transparent. Be able to know who has access to institutional assets and under what conditions.
- In the case of contracts and tenders, you must fill out a conflict of interest questionnaire.
- The selection of the members of the ethics committees should be organized from the bottom up, doctors in higher positions should not be able to influence them.
- The ethical system must be completely independent from the ministry and health institutions, only a court can exercise legal remedies over it.
- The relationship between public and private healthcare must be regulated, and the MOK is also preparing a separate working document on this.